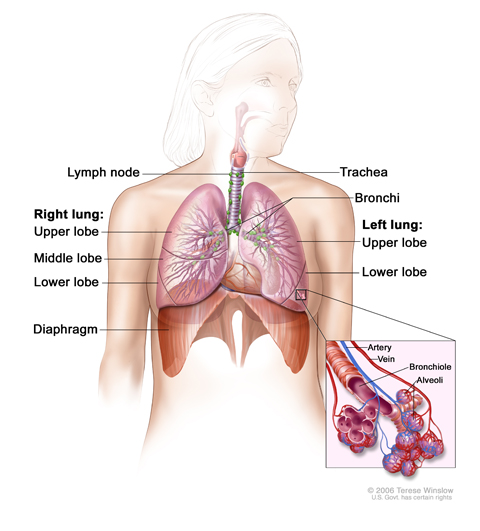
Anatomy of the respiratory system, showing the trachea and both lungs and their lobes and airways. Lymph nodes and the diaphragm are also shown. Oxygen is inhaled into the lungs and passes through the thin membranes of the alveoli and into the bloodstream (see inset).
Non-small cell lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung.
The lungs are a pair of cone-shaped breathing organs in the chest. The lungs bring oxygen into the body as you breathe in. They release carbon dioxide, a waste product of the body’s cells, as you breathe out. Each lung has sections called lobes. The left lung has two lobes. The right lung is slightly larger and has three lobes. Two tubes called bronchi lead from the trachea (windpipe) to the right and left lungs. The bronchi are sometimes also involved in lung cancer. Tiny air sacs called alveoli and small tubes called bronchioles make up the inside of the lungs.
A thin membrane called the pleura covers the outside of each lung and lines the inside wall of the chest cavity. This creates a sac called the pleural cavity. The pleural cavity normally contains a small amount of fluid that helps the lungs move smoothly in the chest when you breathe.
There are several types of non-small cell lung cancer.
Each type of non-small cell lung cancer has different kinds of cancer cells. The cancer cells of each type grow and spread in different ways. The types of non-small cell lung cancer are named for the kinds of cells found in the cancer and how the cells look under a microscope:
Squamous cell carcinoma: Cancer that begins in squamous cells, which are thin, flat cells that look like fish scales. This is also called epidermoid carcinoma.
Large cell carcinoma: Cancer that may begin in several types of large cells.
Adenocarcinoma: Cancer that begins in the cells that line the alveoli and make substances such as mucus.
Other less common types of non-small cell lung cancer are: pleomorphic, carcinoid tumor, salivary gland carcinoma, and unclassified carcinoma.
Smoking is the major risk factor for non-small cell lung cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk to your doctor if you think you may be at risk for lung cancer.
Risk factors for lung cancer include the following:
Smoking cigarettes, pipes, or cigars, now or in the past. This is the most important risk factor for lung cancer. The earlier in life a person starts smoking, the more often a person smokes, and the more years a person smokes, the greater the risk of lung cancer.
Being exposed to secondhand smoke.
Being exposed to radiation from any of the following:
Radiation therapy to the breast or chest.
Radon in the home or workplace.
Imaging tests such as CT scans.
Atomic bomb radiation.
Being exposed to asbestos, chromium, nickel, beryllium, arsenic, soot, or tar in the workplace.
Living where there is air pollution.
Having a family history of lung cancer.
Being infected with the human immunodeficiency virus (HIV).
Taking beta carotene supplements and being a heavy smoker.
Older age is the main risk factor for most cancers. The chance of getting cancer increases as you get older.
When smoking is combined with other risk factors, the risk of lung cancer is increased.
Signs of non-small cell lung cancer include a cough that doesn't go away and shortness of breath.
Sometimes lung cancer does not cause any signs or symptoms. It may be found during a chest x-ray done for another condition. Signs and symptoms may be caused by lung cancer or by other conditions. Check with your doctor if you have any of the following:
Chest discomfort or pain.
A cough that doesn’t go away or gets worse over time.
Trouble breathing.
Wheezing.
Blood in sputum (mucus coughed up from the lungs).
Hoarseness.
Loss of appetite.
Weight loss for no known reason.
Feeling very tired.
Trouble swallowing.
Swelling in the face and/or veins in the neck.
X-ray of the chest. X-rays are used to take pictures of organs and bones of the chest. X-rays pass through the patient onto film.
Tests that examine the lungs are used to detect (find), diagnose, and stage non-small cell lung cancer.
Tests and procedures to detect, diagnose, and stage non-small cell lung cancer are often done at the same time. Some of the following tests and procedures may be used:
Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits, including smoking, and past jobs, illnesses, and treatments will also be taken.
Laboratory tests: Medical procedures that test samples of tissue, blood, urine, or other substances in the body. These tests help to diagnose disease, plan and check treatment, or monitor the disease over time.
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
Sputum cytology: A procedure in which a pathologist views a sample of sputum (mucus coughed up from the lungs) under a microscope, to check for cancer cells.
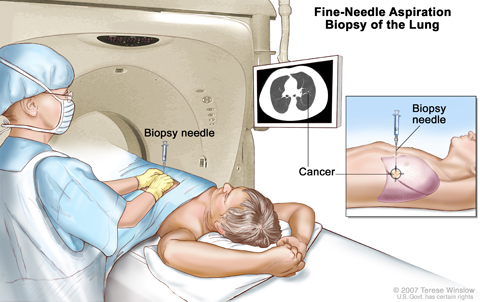
Fine-needle aspiration biopsy of the lung. The patient lies on a table that slides through the computed tomography (CT) machine, which takes x-ray pictures of the inside of the body. The x-ray pictures help the doctor see where the abnormal tissue is in the lung. A biopsy needle is inserted through the chest wall and into the area of abnormal lung tissue. A small piece of tissue is removed through the needle and checked under the microscope for signs of cancer.
Fine-needle aspiration (FNA) biopsy of the lung: The removal of tissue or fluid from the lung using a thin needle. A CT scan, ultrasound, or other imaging procedure is used to locate the abnormal tissue or fluid in the lung. A small incision may be made in the skin where the biopsy needle is inserted into the abnormal tissue or fluid. A sample is removed with the needle and sent to the laboratory. A pathologist then views the sample under a microscope to look for cancer cells. A chest x-ray is done after the procedure to make sure no air is leaking from the lung into the chest.
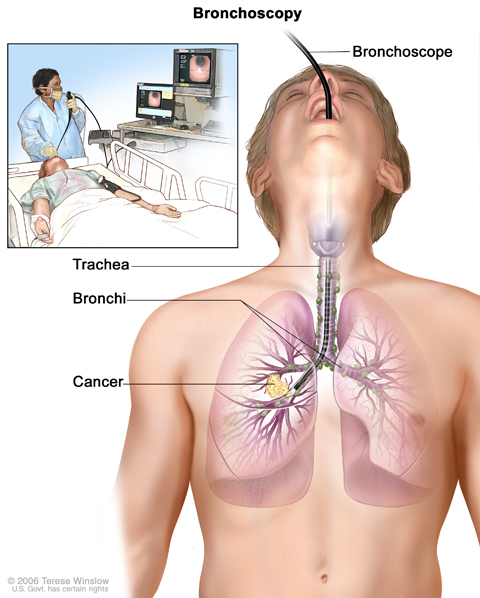
Bronchoscopy. A bronchoscope is inserted through the mouth, trachea, and major bronchi into the lung, to look for abnormal areas. A bronchoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a cutting tool. Tissue samples may be taken to be checked under a microscope for signs of disease.
Bronchoscopy: A procedure to look inside the trachea and large airways in the lung for abnormal areas. A bronchoscope is inserted through the nose or mouth into the trachea and lungs. A bronchoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
Thoracoscopy: A surgical procedure to look at the organs inside the chest to check for abnormal areas. An incision (cut) is made between two ribs, and a thoracoscope is inserted into the chest. A thoracoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of cancer. In some cases, this procedure is used to remove part of the esophagus or lung. If certain tissues, organs, or lymph nodes can’t be reached, a thoracotomy may be done. In this procedure, a larger incision is made between the ribs and the chest is opened.Thoracentesis: The removal of fluid from the space between the lining of the chest and the lung, using a needle. A pathologist views the fluid under a microscope to look for cancer cells.
Light and electron microscopy: A laboratory test in which cells in a sample of tissue are viewed under regular and high-powered microscopes to look for certain changes in the cells.
Immunohistochemistry: A test that uses antibodies to check for certain antigens in a sample of tissue. The antibody is usually linked to a radioactive substance or a dye that causes the tissue to light up under a microscope. This type of test may be used to tell the difference between different types of cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
The stage of the cancer (the size of the tumor and whether it is in the lung only or has spread to other places in the body).
The type of lung cancer.
Whether the cancer has mutations (changes) in certain genes, such as the epidermal growth factor receptor (EGFR) gene or the anaplastic lymphoma kinase (ALK) gene.
Whether there are signs and symptoms such as coughing or trouble breathing.
The patient’s general health.
For most patients with non-small cell lung cancer, current treatments do not cure the cancer.
If lung cancer is found, taking part in one of the many clinical trials being done to improve treatment should be considered. Clinical trials are taking place in most parts of the country for patients with all stages of non-small cell lung cancer. Information about ongoing clinical trials is available from the NCI Web site.
Stages of Non-Small Cell Lung Cancer
After lung cancer has been diagnosed, tests are done to find out if cancer cells have spread within the lungs or to other parts of the body.
The process used to find out if cancer has spread within the lungs or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. Some of the tests used to diagnose non-small cell lung cancer are also used to stage the disease. (See the General Information section.) Other tests and procedures that may be used in the staging process include the following:
MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the brain. This procedure is also called nuclear magnetic resonance imaging (NMRI).
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the brain and abdomen, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
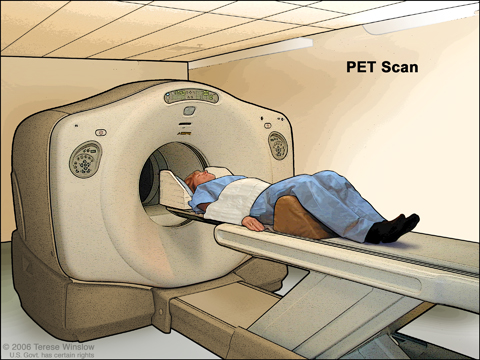
PET (positron emission tomography) scan. The patient lies on a table that slides through the PET machine. The head rest and white strap help the patient lie still. A small amount of radioactive glucose (sugar) is injected into the patient's vein, and a scanner makes a picture of where the glucose is being used in the body. Cancer cells show up brighter in the picture because they take up more glucose than normal cells do.
PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
Radionuclide bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones and is detected by a scanner.
Pulmonary function test (PFT): A test to see how well the lungs are working. It measures how much air the lungs can hold and how quickly air moves into and out of the lungs. It also measures how much oxygen is used and how much carbon dioxide is given off during breathing. This is also called lung function test.
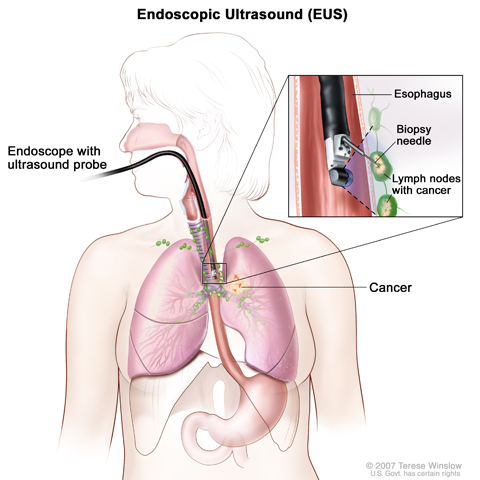
Endoscopic ultrasound-guided fine-needle aspiration biopsy. An endoscope that has an ultrasound probe and a biopsy needle is inserted through the mouth and into the esophagus. The probe bounces sound waves off body tissues to make echoes that form a sonogram (computer picture) of the lymph nodes near the esophagus. The sonogram helps the doctor see where to place the biopsy needle to remove tissue from the lymph nodes. This tissue is checked under a microscope for signs of cancer.
Endoscopic ultrasound (EUS): A procedure in which an endoscope is inserted into the body. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography. EUS may be used to guide fine needle aspiration (FNA) biopsy of the lung, lymph nodes, or other areas.
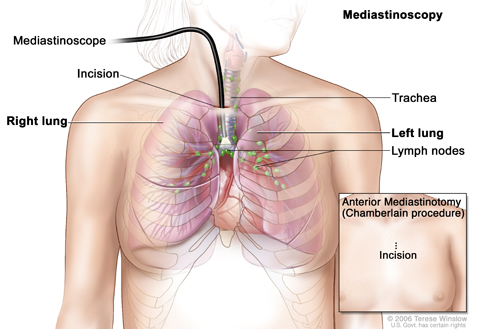
Mediastinoscopy. A mediastinoscope is inserted into the chest through an incision above the breastbone to look for abnormal areas between the lungs. A mediastinoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a cutting tool. Tissue samples may be taken from lymph nodes on the right side of the chest and checked under a microscope for signs of cancer. In an anterior mediastinotomy (Chamberlain procedure), the incision is made beside the breastbone to remove tissue samples from the lymph nodes on the left side of the chest.
Mediastinoscopy: A surgical procedure to look at the organs, tissues, and lymph nodes between the lungs for abnormal areas. An incision (cut) is made at the top of the breastbone and a mediastinoscope is inserted into the chest. A mediastinoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of cancer.
Anterior mediastinotomy: A surgical procedure to look at the organs and tissues between the lungs and between the breastbone and heart for abnormal areas. An incision (cut) is made next to the breastbone and a mediastinoscope is inserted into the chest. A mediastinoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of cancer. This is also called the Chamberlain procedure.
Lymph node biopsy: The removal of all or part of a lymph node. A pathologist views the tissue under a microscope to look for cancer cells.
Bone marrow aspiration and biopsy: The removal of bone marrow, blood, and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to look for signs of cancer.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
Tissue. The cancer spreads from where it began by growing into nearby areas.
Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
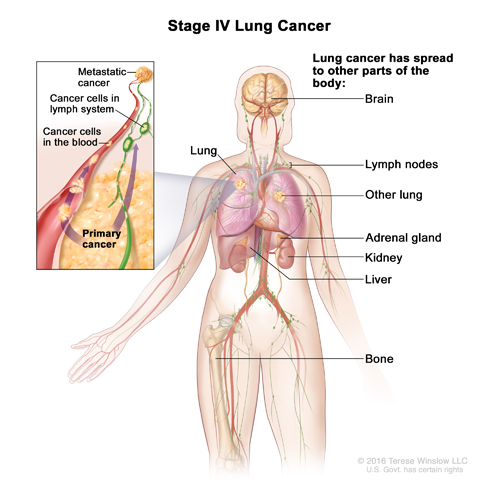
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if non-small cell lung cancer spreads to the brain, the cancer cells in the brain are actually lung cancer cells. The disease is metastatic lung cancer, not brain cancer.
The following stages are used for non-small cell lung cancer:
Occult (hidden) stage
In the occult (hidden) stage, cancer cannot be seen by imaging or bronchoscopy. Cancer cells are found in sputum (mucus coughed up from the lungs) or bronchial washing (a sample of cells taken from inside the airways that lead to the lung). Cancer may have spread to other parts of the body.
Stage 0 (carcinoma in situ)
In stage 0, abnormal cells are found in the lining of the airways. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
Stage I
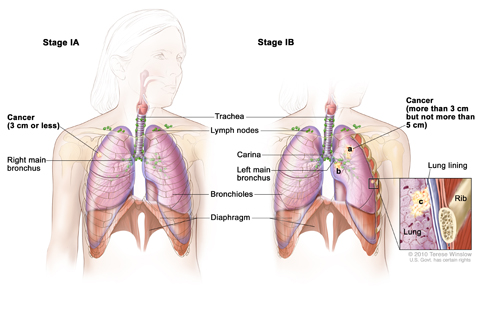
Stage I non-small cell lung cancer. In stage IA, cancer is in the lung only and is 3 cm or smaller. In stage IB, the cancer is (a) larger than 3 cm but not larger than 5 cm, (b) has spread to the main bronchus, and/or (c) has spread to the innermost layer of the lung lining. Part of the lung may have collapsed or become inflamed (not shown).
In stage I, cancer has formed. Stage I is divided into stages IA and IB:
Stage IA: The tumor is in the lung only and is 3 centimeters or smaller.
Stage IB: Cancer has not spread to the lymph nodes and one or more of the following is true:
The tumor is larger than 3 centimeters but not larger than 5 centimeters.
Cancer has spread to the main bronchus and is at least 2 centimeters below where the trachea joins the bronchus.
Cancer has spread to the innermost layer of the membrane that covers the lung.
Part of the lung has collapsed or developed pneumonitis (inflammation of the lung) in the area where the trachea joins the bronchus.
Stage II
Stage II is divided into stages IIA and IIB. Stage IIA and IIB are each divided into two sections depending on the size of the tumor, where the tumor is found, and whether there is cancer in the lymph nodes.
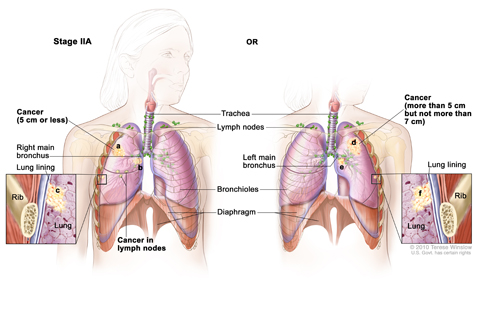
Stage IIA non-small cell lung cancer. Cancer has spread to certain lymph nodes on the same side of the chest as the primary tumor; the cancer is (a) 5 cm or smaller, (b) has spread to the main bronchus, and/or (c) has spread to the innermost layer of the lung lining. OR, cancer has not spread to lymph nodes; the cancer is (d) larger than 5 cm but not larger than 7 cm, (e) has spread to the main bronchus, and/or (f) has spread to the innermost layer of the lung lining. Part of the lung may have collapsed or become inflamed (not shown).
Stage IIA:
(1) Cancer has spread to lymph nodes on the same side of the chest as the tumor. The lymph nodes with cancer are within the lung or near the bronchus. Also, one or more of the following is true:
The tumor is not larger than 5 centimeters.
Cancer has spread to the main bronchus and is at least 2 centimeters below where the trachea joins the bronchus.
Cancer has spread to the innermost layer of the membrane that covers the lung.
Part of the lung has collapsed or developed pneumonitis (inflammation of the lung) in the area where the trachea joins the bronchus.
or
(2) Cancer has not spread to lymph nodes and one or more of the following is true:
The tumor is larger than 5 centimeters but not larger than 7 centimeters.
Cancer has spread to the main bronchus and is at least 2 centimeters below where the trachea joins the bronchus.
Cancer has spread to the innermost layer of the membrane that covers the lung.
Part of the lung has collapsed or developed pneumonitis (inflammation of the lung) in the area where the trachea joins the bronchus.
Stage IIB:
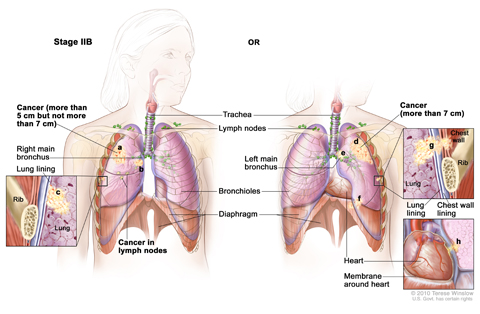
Stage IIB non-small cell lung cancer. Cancer has spread to certain lymph nodes on the same side of the chest as the primary tumor; the cancer is (a) larger than 5 cm but not larger than 7 cm, (b) has spread to the main bronchus, and/or (c) has spread to the innermost layer of the lung lining. Part of the lung may have collapsed or become inflamed (not shown). OR, (d) the cancer is larger than 7 cm; (e) has spread to the main bronchus, (f) the diaphragm, (g) the chest wall or the lining of the chest wall; and/or (h) has spread to the membrane around the heart. There may be one or more separate tumors in the same lobe of the lung; cancer may have spread to the nerve that controls the diaphragm; the whole lung may have collapsed or become inflamed (not shown).
(1) Cancer has spread to nearby lymph nodes on the same side of the chest as the tumor. The lymph nodes with cancer are within the lung or near the bronchus. Also, one or more of the following is true:
The tumor is larger than 5 centimeters but not larger than 7 centimeters.
Cancer has spread to the main bronchus and is at least 2 centimeters below where the trachea joins the bronchus.
Cancer has spread to the innermost layer of the membrane that covers the lung.
Part of the lung has collapsed or developed pneumonitis (inflammation of the lung) in the area where the trachea joins the bronchus.
or
(2) Cancer has not spread to lymph nodes and one or more of the following is true:
The tumor is larger than 7 centimeters.
Cancer has spread to the main bronchus (and is less than 2 centimeters below where the trachea joins the bronchus), the chest wall, the diaphragm, or the nerve that controls the diaphragm.
Cancer has spread to the membrane around the heart or lining the chest wall.
The whole lung has collapsed or developed pneumonitis (inflammation of the lung).
There are one or more separate tumors in the same lobe of the lung.
Stage IIIA
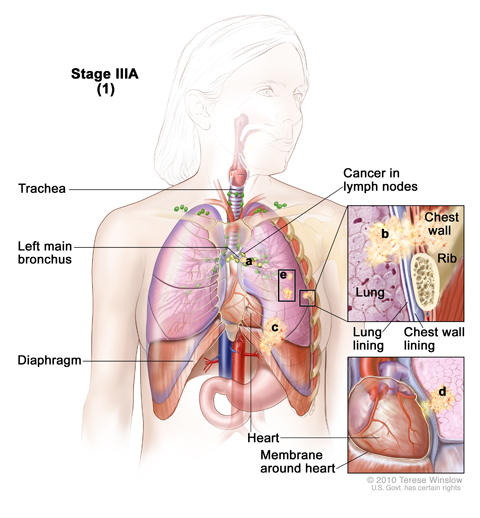
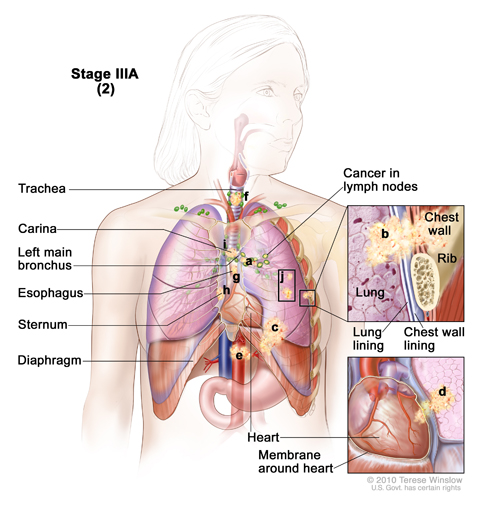
Stage IIIA non-small cell lung cancer (1). Cancer has spread to certain lymph nodes on the same side of the chest as the primary tumor. The cancer may have spread to (a) the main bronchus; (b) lung lining, chest wall lining, or chest wall; (c) diaphragm; and/or (d) membrane around the heart; and/or (e) there may be one or more separate tumors in the same lobe of the lung. Cancer may have spread to the nerve that controls the diaphragm, and part or all of the lung may have collapsed or become inflamed (not shown).
Stage IIIA is divided into three sections depending on the size of the tumor, where the tumor is found, and which lymph nodes have cancer (if any).
(1) Cancer has spread to lymph nodes on the same side of the chest as the tumor. The lymph nodes with cancer are near the sternum (chest bone) or where the bronchus enters the lung. Also:
The tumor may be any size.
Part of the lung (where the trachea joins the bronchus) or the whole lung may have collapsed or developed pneumonitis (inflammation of the lung).
There may be one or more separate tumors in the same lobe of the lung.
Cancer may have spread to any of the following:
Main bronchus, but not the area where the trachea joins the bronchus.
Chest wall.
Diaphragm and the nerve that controls it.
Membrane around the lung or lining the chest wall.
Membrane around the heart.
or
Stage IIIA lung cancer (2)
Cancer has spread to certain lymph nodes on the same side of the chest as the primary tumor. The cancer may have spread to (a) the main bronchus; (b) the lung lining, chest wall lining, or chest wall; (c) diaphragm; (d) heart and/or membrane around the it; (e) major blood vessels that lead to or from the heart; (f) trachea; (g) esophagus; (h) sternum; and/or (i) carina; and/or (j) there may be one or more separate tumors in any lobe of the same lung. Cancer may have spread to the nerves that control the diaphragm and larynx, and the whole lung may have collapsed or become inflamed (not shown).
(2) Cancer has spread to lymph nodes on the same side of the chest as the tumor. The lymph nodes with cancer are within the lung or near the bronchus. Also:
The tumor may be any size.
The whole lung may have collapsed or developed pneumonitis (inflammation of the lung).
There may be one or more separate tumors in any of the lobes of the lung with cancer.
Cancer may have spread to any of the following:
Main bronchus, but not the area where the trachea joins the bronchus.
Chest wall.
Diaphragm and the nerve that controls it.
Membrane around the lung or lining the chest wall.
Heart or the membrane around it.
Major blood vessels that lead to or from the heart.
Trachea.
Esophagus.
Nerve that controls the larynx (voice box).
Sternum (chest bone) or backbone.
Carina (where the trachea joins the bronchi).
or
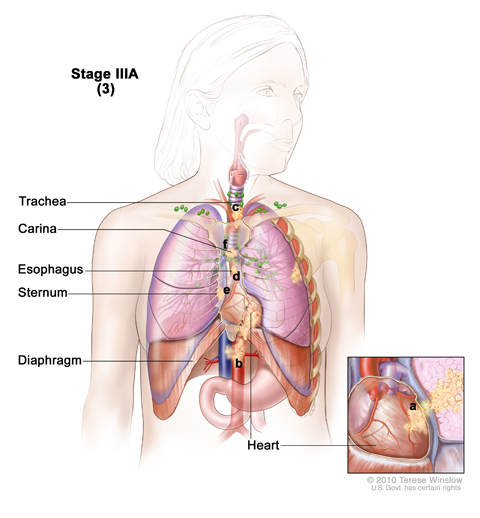
Stage IIIA non-small cell lung cancer (3). Cancer has spread to (a) the heart; (b) major blood vessels that lead to or from the heart; (c) trachea; (d) esophagus; (e) sternum; and/or (f) carina. Cancer may have spread to the nerve that controls the larynx (not shown).
(3) Cancer has not spread to the lymph nodes and the tumor may be any size. Cancer has spread to any of the following:
Heart.
Major blood vessels that lead to or from the heart.
Trachea.
Esophagus.
Nerve that controls the larynx (voice box).
Sternum (chest bone) or backbone.
Carina (where the trachea joins the bronchi).
Stage IIIB
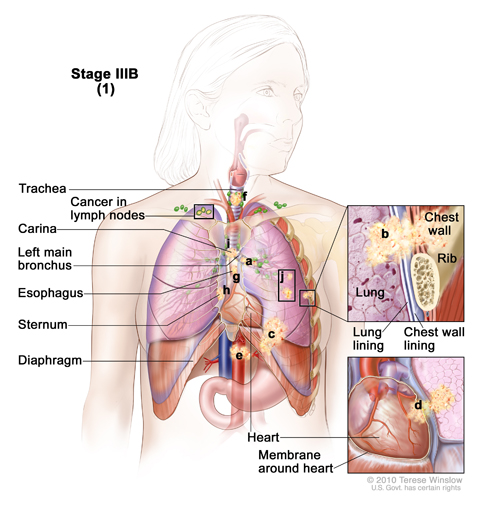
Stage IIIB non-small cell lung cancer (1). Cancer has spread to lymph nodes above the collarbone or on the opposite side of the chest as the primary tumor. The cancer may have spread to (a) the main bronchus; (b) lung lining, chest wall lining, or chest wall; (c) diaphragm; (d) heart or the membrane around it; (e) major blood vessels that lead to or from the heart; (f) trachea; (g) esophagus; (h) sternum; and/or (i) carina; and/or (j) there may be one or more separate tumors in any of the lobes of the lung. Part or all of the lung may have collapsed or become inflamed and cancer may have spread to the backbone and/or the nerves that control the diaphragm and larynx (not shown).
Stage IIIB is divided into two sections depending on the size of the tumor, where the tumor is found, and which lymph nodes have cancer.
(1) Cancer has spread to lymph nodes above the collarbone or to lymph nodes on the opposite side of the chest as the tumor. Also:
The tumor may be any size.
Part of the lung (where the trachea joins the bronchus) or the whole lung may have collapsed or developed pneumonitis (inflammation of the lung).
There may be one or more separate tumors in any of the lobes of the lung with cancer.
Cancer may have spread to any of the following:
Main bronchus.
Chest wall.
Diaphragm and the nerve that controls it.
Membrane around the lung or lining the chest wall.
Heart or the membrane around it.
Major blood vessels that lead to or from the heart.
Trachea.
Esophagus.
Nerve that controls the larynx (voice box).
Sternum (chest bone) or backbone.
Carina (where the trachea joins the bronchi).
or
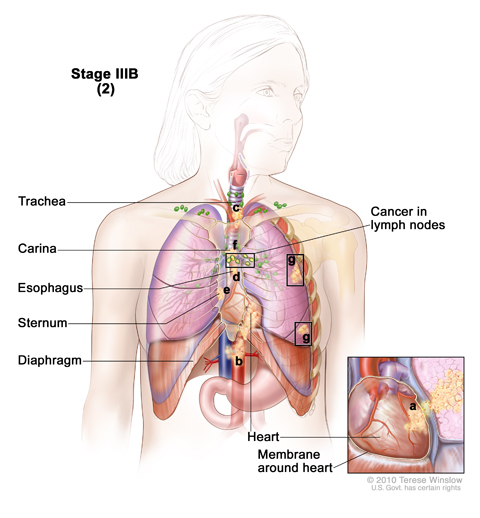
Stage IIIB non-small cell lung cancer
Cancer has spread to certain lymph nodes on the same side of the chest as the primary tumor and to (a) the heart; (b) major blood vessels that lead to or from the heart; (c) trachea; (d) esophagus; (e) sternum; and/or (f) carina; and/or (g) there may be separate tumors in different lobes of the same lung. Cancer may have spread to the backbone and/or the nerve that controls the larynx (not shown).
(2) Cancer has spread to lymph nodes on the same side of the chest as the tumor. The lymph nodes with cancer are near the sternum (chest bone) or where the bronchus enters the lung. Also:
The tumor may be any size.
There may be separate tumors in different lobes of the same lung.
Cancer has spread to any of the following:
Heart.
Major blood vessels that lead to or from the heart.
Trachea.
Esophagus.
Nerve that controls the larynx (voice box).
Sternum (chest bone) or backbone.
Carina (where the trachea joins the bronchi).
Stage IV
Stage IV non-small cell lung cancer. The cancer has spread to the other lung, and/or to lymph nodes, fluid around the lungs or heart, and/or other parts of the body, such as the brain, liver, adrenal gland, kidney, or bone.
In stage IV, the tumor may be any size and cancer may have spread to lymph nodes. One or more of the following is true:
There are one or more tumors in both lungs.
Cancer is found in fluid around the lungs or the heart.
Cancer has spread to other parts of the body, such as the brain, liver, adrenal glands, kidneys, or bone.
Recurrent Non-Small Cell Lung Cancer
Recurrent non-small cell lung cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the brain, lung, or other parts of the body.
Treatment Option Overview
There are different types of treatment for patients with non-small cell lung cancer.
Different types of treatments are available for patients with non-small cell lung cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Nine types of standard treatment are used:
Surgery
Four types of surgery are used to treat lung cancer:
Wedge resection: Surgery to remove a tumor and some of the normal tissue around it. When a slightly larger amount of tissue is taken, it is called a segmental resection.
Lobectomy: Surgery to remove a whole lobe (section) of the lung.
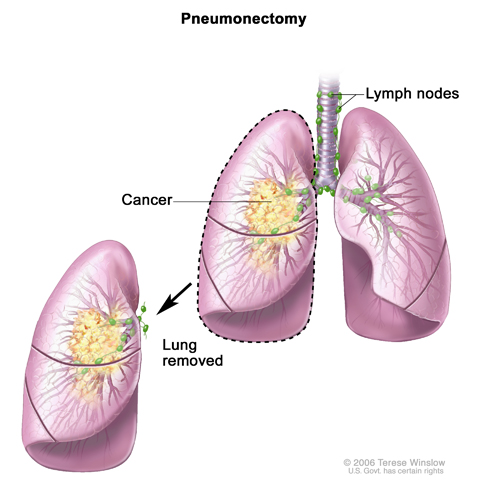
Pneumonectomy. The whole lung is removed.
Pneumonectomy: Surgery to remove one whole lung.
Sleeve resection: Surgery to remove part of the bronchus.
Even if the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
Radiosurgery is a method of delivering radiation directly to the tumor with little damage to healthy tissue. It does not involve surgery and may be used to treat certain tumors in patients who cannot have surgery.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. It also depends on where the cancer is found. For tumors in the airways, radiation is given directly to the tumor through an endoscope.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Targeted therapy is a type of treatment that uses drugs or other substances to attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do. Monoclonal antibodies and small-molecule tyrosine kinase inhibitors are the two main types of targeted therapy being used in the treatment of non-small cell lung cancer.
Monoclonal antibody therapy is a cancer treatment that uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances in the blood or tissues that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Monoclonal antibodies used to treat non-small cell lung cancer include bevacizumab and cetuximab. Bevacizumab binds to vascular endothelial growth factor (VEGF) in the blood and tissues and may prevent the growth of new blood vessels that tumors need to grow. Cetuximab is a monoclonal antibody that acts as a tyrosine kinase inhibitor. It binds to epidermal growth factor receptor (EGFR), which is a tyrosine kinase protein, on the surface of cancer cells and works to stop the cells from growing and dividing.
Small-molecule tyrosine kinase inhibitors are targeted therapy drugs that work inside cancer cells and block signals needed for tumors to grow. Small-molecule tyrosine kinase inhibitors may be used with other anticancer drugs as adjuvant therapy.
Small-molecule tyrosine kinase inhibitors used to treat non-small cell lung cancer include erlotinib and gefitinib. They are types of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors.
Crizotinib is another type of small-molecule tyrosine kinase inhibitor that is used to treat non-small cell lung cancer. It is used to treat non-small cell lung cancer that has certain mutations (changes) in the anaplastic lymphoma kinase (ALK) gene. The protein made by the ALK gene has tyrosine kinase activity.
Laser therapy is a cancer treatment that uses a laser beam (a narrow beam of intense light) to kill cancer cells.
Photodynamic therapy (PDT)
Photodynamic therapy (PDT) is a cancer treatment that uses a drug and a certain type of laser light to kill cancer cells. A drug that is not active until it is exposed to light is injected into a vein. The drug collects more in cancer cells than in normal cells. Fiberoptic tubes are then used to carry the laser light to the cancer cells, where the drug becomes active and kills the cells. Photodynamic therapy causes little damage to healthy tissue. It is used mainly to treat tumors on or just under the skin or in the lining of internal organs. When the tumor is in the airways, PDT is given directly to the tumor through an endoscope.
Cryosurgery
Cryosurgery is a treatment that uses an instrument to freeze and destroy abnormal tissue, such as carcinoma in situ. This type of treatment is also called cryotherapy. For tumors in the airways, cryosurgery is done through an endoscope.
Electrocautery
Electrocautery is a treatment that uses a probe or needle heated by an electric current to destroy abnormal tissue. For tumors in the airways, electrocautery is done through an endoscope.
Watchful waiting
Watchful waiting is closely monitoring a patient’s condition without giving any treatment until signs or symptoms appear or change. This may be done in certain rare cases of non-small cell lung cancer.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI Web site.
Chemoprevention
Chemoprevention is the use of drugs, vitamins, or other substances to reduce the risk of cancer or to reduce the risk cancer will recur (come back).
New combinations
New combinations of treatments are being studied in clinical trials.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. See the Treatment Options section that follows for links to current treatment clinical trials. These have been retrieved from NCI's listing of clinical trials.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Treatment Options by Stage
Occult Non-Small Cell Lung Cancer
Treatment of occult non-small cell lung cancer depends on the stage of the disease. Occult tumors are often found at an early stage (the tumor is in the lung only) and sometimes can be cured by surgery.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with occult non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage 0 (Carcinoma in Situ)
Treatment of stage 0 may include the following:
Surgery (wedge resection or segmental resection).
Photodynamic therapy using an endoscope.
Electrocautery, cryosurgery, or laser surgery using an endoscope.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage 0 non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage I Non-Small Cell Lung Cancer
Treatment of stage I non-small cell lung cancer may include the following:
Surgery (wedge resection, segmental resection, sleeve resection, or lobectomy).
External radiation therapy (for patients who cannot have surgery or choose not to have surgery).
A clinical trial of chemotherapy or radiation therapy following surgery.
A clinical trial of surgery followed by chemoprevention.
A clinical trial of treatment given through an endoscope, such as photodynamic therapy (PDT).
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage I non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage II Non-Small Cell Lung Cancer
Treatment of stage II non-small cell lung cancer may include the following:
Surgery (wedge resection, segmental resection, sleeve resection, lobectomy, or pneumonectomy).
Chemotherapy followed by surgery.
Surgery followed by chemotherapy.
External radiation therapy (for patients who cannot have surgery or choose not to have surgery).
A clinical trial of radiation therapy following surgery.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage II non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage IIIA Non-Small Cell Lung Cancer
Treatment of stage IIIA non-small cell lung cancer that can be removed with surgery may include the following:
Surgery followed by chemotherapy.
Chemotherapy followed by surgery.
Surgery followed by chemotherapy combined with radiation therapy.
Surgery followed by radiation therapy.
A clinical trial of new combinations of treatments.
Treatment of stage IIIA non-small cell lung cancer that cannot be removed with surgery may include the following:
Chemotherapy and radiation therapy given as separate treatments over the same period of time.
External radiation therapy alone (for patients who cannot be treated with combined therapy, as palliative treatment to relieve symptoms and improve the quality of life).
Internal radiation therapy or laser surgery, as palliative treatment to relieve symptoms and improve the quality of life.
A clinical trial of new combinations of treatments.
For more information about supportive care for signs and symptoms including cough, shortness of breath, and chest pain, see the PDQ summary on Cardiopulmonary Syndromes.
Non-small cell lung cancer of the superior sulcus, often called Pancoast tumor, begins in the upper part of the lung and spreads to nearby tissues such as the ribs and vertebrae. Treatment of Pancoast tumors may include the following:
Radiation therapy alone.
Radiation therapy followed by surgery.
Chemotherapy and radiation therapy given as separate treatments over the same period of time, followed by surgery.
Surgery alone.
A clinical trial of new combinations of treatments.
Some stage IIIA non-small cell lung tumors that have grown into the chest wall may be completely removed. Treatment of chest wall tumors may include the following:
Surgery.
Surgery and radiation therapy.
Radiation therapy alone.
Chemotherapy combined with radiation therapy and/or surgery.
A clinical trial of new combinations of treatments.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage III non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage IIIB Non-Small Cell Lung Cancer
Treatment of stage IIIB non-small cell lung cancer may include the following:
Chemotherapy followed by external radiation therapy.
Chemotherapy and radiation therapy given as separate treatments over the same period of time.
Chemotherapy followed by surgery.
External radiation therapy alone for patients who cannot be treated with chemotherapy.
External or internal radiation therapy as palliative therapy, to relieve pain and other symptoms and improve the quality of life.
Clinical trials of new radiation therapy schedules and new combinations of treatments.
For more information about supportive care for signs and symptoms such as cough, shortness of breath, and chest pain, see the following PDQ summaries:
Cardiopulmonary Syndromes
Pain
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage III non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Stage IV Non-Small Cell Lung Cancer
Treatment of stage IV non-small cell lung cancer may include the following:
Combination chemotherapy.
Maintenance therapy with an anticancer drug to help keep cancer from progressing, after combination chemotherapy.
Combination chemotherapy and targeted therapy with a monoclonal antibody, such as bevacizumab or cetuximab.
Targeted therapy with a small-molecule tyrosine kinase inhibitor, such as erlotinib or crizotinib.
External radiation therapy as palliative therapy, to relieve pain and other symptoms and improve the quality of life.
Laser therapy and/or internal radiation therapy.
A clinical trial of new drugs and combinations of treatments.
For more information about supportive care for signs and symptoms including cough, shortness of breath, and chest pain, see the following PDQ summaries:
Cardiopulmonary Syndromes
Pain
Check the list of NCI-supported cancer clinical trials that are now accepting patients with stage IV non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
Treatment Options for Recurrent Non-Small Cell Lung Cancer
Treatment of recurrent non-small cell lung cancer may include the following:
External radiation therapy as palliative therapy, to relieve pain and other symptoms and improve the quality of life.
Chemotherapy.
Targeted therapy with a small-molecule tyrosine kinase inhibitor, such as erlotinib or crizotinib.
Laser therapy or internal radiation therapy using an endoscope.
Radiosurgery (for certain patients who cannot have surgery).
Surgery to remove a very small amount of cancer that has spread to the brain.
Check the list of NCI-supported cancer clinical trials that are now accepting patients with recurrent non-small cell lung cancer. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your doctor about clinical trials that may be right for you. General information about clinical trials is available from the NCI website.
To Learn More About Non-Small Cell Lung Cancer
For more information from the National Cancer Institute about non-small cell lung cancer, see the following:


 Wedge resection: Surgery to remove a tumor and some of the normal tissue around it. When a slightly larger amount of tissue is taken, it is called a segmental resection.
Wedge resection: Surgery to remove a tumor and some of the normal tissue around it. When a slightly larger amount of tissue is taken, it is called a segmental resection.