
How are the nipple and areola reconstructed during breast surgery?
-
The nipple and areola are key elements of the reconstructed breast after mastectomy and are essential in restoring the breast to its natural form. Many patients have questions about how and when the nipple and areola are reconstructed. The first step in breast reconstruction is to create a breast mound. This is accomplished using implants or the patient’s own tissue or a combination of both. Revisions to the breast mound may be required in each of these circumstances to form a natural breast shape. Once the breast mound is completed, nipple and areola reconstruction beings. Typically, the nipple is reconstructed first followed by the areola. There may be some variation in the timing of nipple areola reconstruction depending on the need for radiation and chemotherapy.
Nipple reconstruction
Once the breast mound is stable nipple reconstruction begins. In most cases this process begins once chemotherapy and radiation are completed. If no radiation is required, nipple reconstruction is performed 3 months after reconstruction of the breast mound is completed. If a patient has been radiated they may wait up to 6 months prior to nipple reconstruction. This delay after radiation allows the skin to heal and reduces the risk of complications. Radiation can also change the shape of the breast mound. Waiting for 6 months allows the nipple to be placed in the correct position and improves symmetry between breasts. After a patient has received radiation the reconstructed nipple may have less projection than in non-radiated patients. There is also a higher risk of wound separation and delayed wound healing.
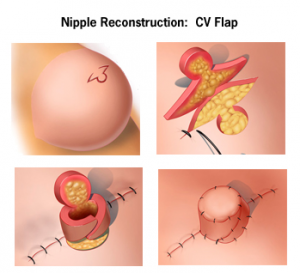
Selection of the new nipple location on the breast mound is an essential part of obtaining a symmetrical appearance. This is accomplished by localizing the nipple position with measurements on each breast. There are a variety of methods used to reconstruct the nipple. In most techniques the local tissue is surgically elevated, folded on itself and sutured to itself to hold the new nipple in place. Reconstructed nipples have a tendency to shrink up to 50 percent of their original size during wound healing. The nipple is often created with greater projection and size then the desired nipple to accommodate shrinkage.

In some methods nipple reconstruction is combined with areola reconstruction using skin grafting. First, the nipple is created then skin from the groin or abdominal wall is transferred to the breast fitting over the nipple in the shape of a doughnut. Skin grafting techniques such as these are used less frequently today and are being replaced by areola and nipple tattooing. Sutures used to hold the reconstructed nipple together are removed two weeks after surgery and allowed to heal for 3 months prior to areola tattooing. Once healed, the surgically created nipple does not change in size or shape with arousal or changes in temperature like natural nipples. They also offer no erotic or normal skin sensation. Reconstructed nipples have a very realistic appearance and act as a landmark for the breast making the reconstructed breast look natural and aesthetically pleasing.